
Have you ever thought about how long it would take you to get to a health center if you had an emergency? It is estimated that one in three people in the region have unmet health needs. And while it is true that not all access depends on infrastructure, it is important to extend access to health services.
Technology now makes it possible to combine layers of population datawith layers of infrastructure to determine how many people are isolated from health services in the region due to infrastructure. Using IDB’s health infrastructure visualizer, we identified how health centers are distributed in 16 countries in the region and how much time and distance separate some communities from receiving medical care. Here are some of the lessons learned from this analysis.
The Availability of Health Centers Varies from Country to Country
WHO data from 2013 show that Mexico, Suriname and Guyana have higher rates of health centers (hospitals, health centers and health posts) per capita – with 105.6, 46.9 and 45.8 hospitals per 100,000 inhabitants – while Haiti, Jamaica, Ecuador and Costa Rica report less than one health center per 100,000 inhabitants.
If we think about emergency situations, how long is a long time to get to a health center? 30 minutes sounds reasonable, doesn’t it?
For the following analysis, we collected official data in 16 countries in the region for a total of 250,000 health facilities, including hospitals, clinics and primary care units (see Map 1). Note that the data should be interpreted with caution given the variability in size and level of service of health facilities across countries.
Map 1. Population and isochrones

Source: Data collected by the Inter-American Development Bank (IDB). Data available on the IDB’s Social Data digital platform. High-resolution population density data from Data for Good at Meta and data on health centers published by the Ministry of Health or the government entity in charge are used. In Argentina we use the list of health facilities registered in the Federal Registry (REFES), in Bolivia the list of first level health facilities of the Ministry of Health, in Brazil the data from the Cadastro Nacional de Estabelecimentos de Saúde (CNES), in Chile the list of health facilities of the Ministry of Health, in Colombia, data on health care institutions (IPS) from the Special Registry of Health Service Providers and Sites (REPS); in Ecuador, the list of health facilities at the national level from the Ministry of Health; in El Salvador, the list of basic, intermediate and specialized community family health units (UCSF); in Guatemala, we used the list of hospitals from the Ministry of Health provided directly to IDB specialists, in Guyana the list of health centers, regional and district hospitals and diagnostic centers of the Ministry of Health, in Haiti the list of health centers constructed by USAID and PAHO, in Honduras we used the list of hospitals of the Ministry of Health provided directly to IDB specialists, in Jamaica hospitals and health centers of the Ministry of Health, in Mexico the list of CLUES health facilities from the Dirección General de Información en Salud (DGIS), in Peru the list of health facilities from the Ministry of Health, in the Dominican Republic the list of health facilities from the Ministry of Health, and in Trinidad and Tobago the list of health centers and public hospitals from the Ministry of Health.
Here we can see in orange the areas whose population must drive at least 30 minutes to reach a health center: out of a total of 586 million people, about 55 million or 9.4% -equivalent to almost the entire population of Argentina.
These results are even more pronounced in Colombia, Honduras and Guatemala, where about 25% of the population lacks access to health centers within a 30-minute drive, and in Peru, where this figure reaches 15%.
In other countries, the figures are more encouraging: it is estimated that in Trinidad and Tobago, Jamaica and Chile, about 0.6%, 0.7% and 3.4%, respectively, of people do not have access to health centers within a 30-minute drive (see Graph 2).
Percentage of people without access to medical centers within a 30-minute radius (%)
How to Use This Information to Extend the Offer of Health Services?
We identified the areas at the municipal level with the highest number of people without access to health centers. Approximately 21 million people (3.6% of the regional population) live in municipalities with rates of lack of access above 50%. These results are more pronounced in Guatemala and Colombia, with 8.5 million (17% of their population) and 3.1 million (18% of their population) respectively, living in municipalities with high rates of lack of access.
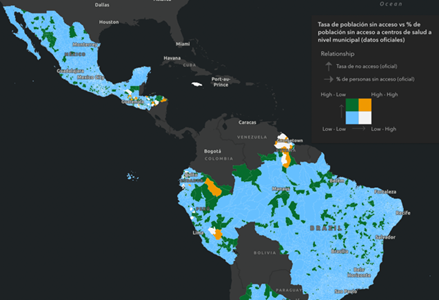
Population density is a factor to take into account: of this group of people without access, 11.5 million live in municipalities with higher density. In Honduras, for example, 1.1 million people are located in the 95 municipalities where the rate of lack of access is at least 50%. Map 2 shows on the left side those municipalities that have the highest rates of non-access to health services; however, the map on the right shows in orange the municipalities that have lack of access but also have relatively high population concentration. Both maps can be viewed in more detail at the following link.
Map 2. Distribution of access to health care and population density.
% of people without access to health centers of the total number of people in each municipality

Municipalities with the highest % of people without access: in orange the high priority areas to improve access
Economic factors also play a crucial role. When comparing access data with poverty rates, we find a clear correlation (see poverty map here). Among municipalities with higher poverty rates, the lack of access to health services is more accentuated, reaching an average of 27%, compared to 11% in municipalities in the lowest poverty quintile.
Moreover, municipalities classified within the 40% with the highest poverty rates concentrate 19% of the regional population, 33% of the population in poverty and an overwhelming 48% of the population without access to health services within a 30-minute drive. These results are more pronounced in Brazil, Peru, Jamaica, Dominican Republic, and Argentina (see Figure 3), where at least 45% of the population without access resides in municipalities with poverty rates of at least 40%, compared to the population without access in municipalities with lower poverty rates.
Percentage of people without access by level of poverty
This analysis sheds light on the complex interaction between social infrastructure and the well-being of people in the region and provides an example of the value of time and distance analysis for decision making. However, this is a first approximation of the potential of this type of analysis. Other variables, such as the care capacity of each center, the quality and timeliness of care, need to be considered, but we hope that this is a beginning of more in-depth studies with geospatial information in the region.
If you want to further explore social infrastructure data and maps in the region, we invite you to access the Social Data digital platform and map viewer here. To participate in the social infrastructure conversation, contribute data or discuss improvements in the ongoing analysis of social infrastructure in Latin America and the Caribbean, leave us your comments below or write to us at [email protected] and [email protected]. Your collaboration is critical to enrich our understanding and promote significant improvements in social infrastructure in the region!
Leave a Reply